A snippet of omgyno's social impact
Words by Dr. Eliannore Boutros, program manager at omgyno and family medicine resident physician
It was mid-October 2024, and the war in Lebanon had escalated. Bombings had become part of daily life, and thousands sought refuge in overcrowded shelters across the country. We were all living in constant uncertainty, glued to our phones, waiting for the next piece of bad news. Functioning felt impossible. We kept asking ourselves how we could possibly continue our work when everything around us seemed so fragile.
Due to limited resources, many SRHR responses had to be selective at the time. Yet when a woman in need stands before you, telling her that her care is conditional feels like denying her dignity.
One day, our Instagram page pinged with a message from a woman we’ll call “D,” who had opened a shelter in Hazmieh, and received over 200 migrant domestic workers mostly from Sierra Leone. She asked if we had a mobile clinic. We immediately had one of those ideas that makes everyone roll their eyes—and then roll up their sleeves. “Hold on,” we said. “We can do so much better.”

Building a system from scratch
I’m really fortunate to work with people who run toward challenges when most would walk away. That same day, we started sketching a plan: what if we could screen every woman in that shelter, test those who needed it, and offer teleconsultations? It sounded nearly impossible. The timeline was tight, the logistics demanding, and the stakes high. But the thing about our team is that when you say “no,” someone always asks, “why not?”
For the next two weeks, we lived on adrenaline. Dimagi offered us a free subscription to CommCare, a HIPAA-compliant platform built for humanitarian field work. Meedan offered to financially support our intervention. Dr. Sarab El Samad helped us design a simple triage system that anyone could use, even without medical training. Doreen and Rosa built the algorithm on CommCare, linking every step of the process, from registration to teleconsultation, and refined it by day and by night. And the rest of the team handled logistics: sourcing kits, coordinating with the lab, printing multilingual instructions, and running an online donation campaign. We barely slept, argued plenty, but kept moving. There wasn’t time for hesitation, only for making it happen.
Our Two Days in Hazmieh
We arrived at the shelter unsure of what to expect. The atmosphere was tense, but there was a quiet sense of purpose among everyone there. We had community health workers (CHWs) ready to help, though we’d never met before.
Day One was about training. We guided the CHWs on how to use CommCare, conduct the triage, and flag anyone needing immediate intervention or follow-up. By the end of the day, every woman in the shelter was registered on the platform, and the CHWs were confidently navigating a system they had just learned.
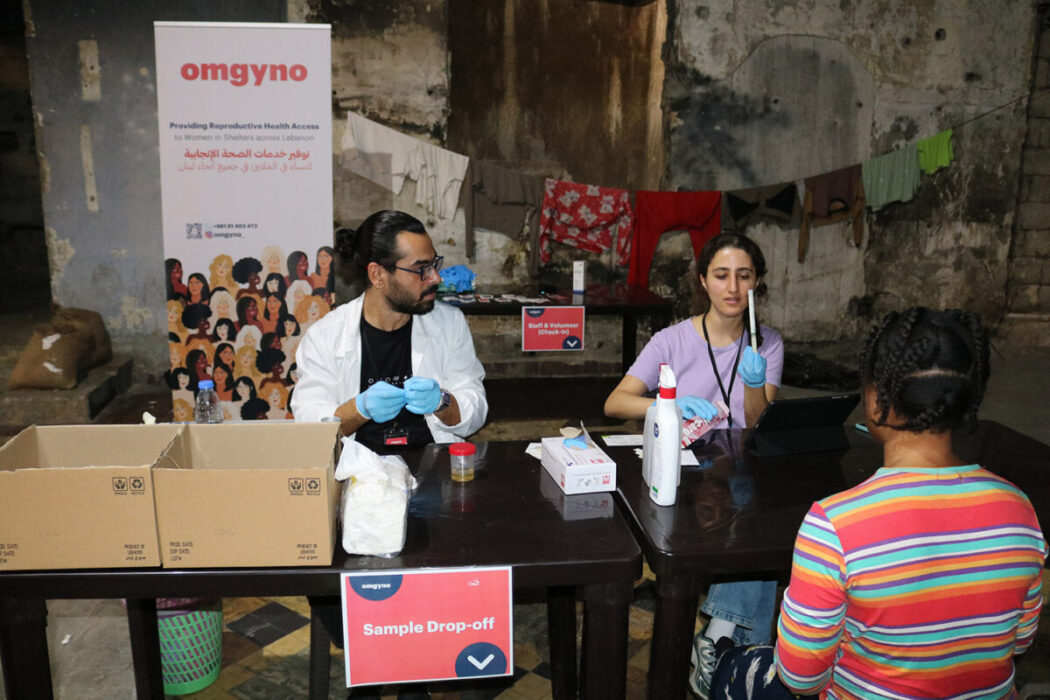
Day Two was when it all came together. We turned part of the shelter into a small clinic with three stations: registration, test pickup and instructions, and sample drop-off.
Those who needed follow-up met Dr. Sarab via Zoom from France.
In a quiet corner of the shelter, they spoke to a doctor abroad while bombs echoed in the distance. It was a brief moment of calm within chaos, a quiet reminder of why we do this work.